Posted November 25th 2014
*The outbreaks of Ebola Virus Disease (EVD) in Senegal and Nigeria were declared over on 17 October and 19 October 2014, respectively. A national EVD outbreak is considered to be over when 42 days (double the 21-day incubation period of the Ebola virus) has elapsed since the last patient in isolation became laboratory negative for EVD.
Originally posted on Sunday October 19, 2014
Ebola e-Control vs. Ebola Ebullience: How to Implement Comprehensive Proactive Preventative Measures, Rather than Reactive Measures to Control the Ebola Epidemic and Avoid Law Suits from Potential Victims
By
Shree Vinekar, MD and A. V. Lakshminarayanan, PhD
First we should seriously acknowledge that Ebola infection is a terrible disease. We should not proclaim "we will stop Ebola in its tracks", which is a most vapid statement, to say the least. To say such things conveys an air of superiority over a mere virus and a sense of shortsightedness when dealing with a potential epidemic.
We do not have a full understanding of its lethal potential, virulent actions and preventive measures we should take, though the Center for Disease Control (CDC) is sincerely trying to gain some deeper understanding of these issues at the eleventh hour. However, as yet, we do not know its "tracks" – indeed, now the tracks are all over the US.
There are many assumptions being made about the spread of the disease. Some of the most important of these unknowns are:
We fail to entertain the thought that fever levels and symptom levels can be
vastly different,
particularly from continent to continent, race to race, and also individual to individual, leave
alone the complexity of differential diagnoses of mild pyrexia. Triaging all patients with elevated
body temperature unnecessarily burdens the front line health care workers with a major dilemma.
This burden arises when thousands of people all over the country present with fever in
front line medical clinics and emergency rooms. Therefore, there need to be more specific criteria with
bio markers, if at all possible, to promptly implement detection and facilitate correct diagnosis of Ebola infection on all frontiers of health care, including public and private health care facilities.
Have we forgotten the history of "Typhoid Mary" in dealing with Ebola? Many "contacts" could be infectious a few days before they manifest recognizable symptoms of the Ebola infection not to mention that not all contacts will become alert enough to the dangers of the infection in a timely fashion to present themselves in a clinic or medical emergency room. There very well could be carriers of Ebola like, "typhoid Mary," who could go undetected as carriers until it is too late. Such dangers speak against complacence in our current ability to "stop Ebola in its tracks." The fact that 50% of the exposed individuals do not manifest illness of "Ebola infection" is in itself a red flag indicating the likelihood that many infectious persons may be running loose in society since having been already exposed to this virus.
One can very well understand the politically correct attitude of the government in not wanting to spread
panic while simultaneously providing primary and secondary prevention as well as excellent tertiary prevention and tertiary treatment centers all around the country. Even in this effort, however, the public is not entirely trusting of the governmental agencies responsible for this task.
Many individuals who were unfortunate to be on the same airplane as the Ebola patients likely feel they are not properly and promptly identified, nor given adequate information, nor sufficiently protected from the ensuing harm. Indeed, this feeling will linger at least for 21days, which is now strongly believed to be the incubation period for this infectious disease.
For example, the poor nurse who later tested positive for the Ebola infection, but who had been cleared for air travel by the CDC was sitting in the aisle in the airplane. Many other passengers could have rubbed against her if she was sitting in the aisle. Indeed, had she been sitting in a window or middle seat, it would have been nearly impossible to not come in contact with her fellow seatmates. Regardless, it was an act of commission with full knowledge that she was a participant in providing care for an Ebola victim.
And, yet, to isolate, quarantine, and monitor only those who sat close to the stricken nurse in the plane is very near-sighted. If she went to the toilet facilities, in the airplane or at the airports, very many more should be watched. Also what happened to the cups or utensils used by the person, either in the aircraft or at the airports? There are many more aspects to this specific public health expertise related skills that are simply dictated by common sense, that the people involved in guarding the public health in this country seem to be direly lacking in them or have not demonstrated that they possess these. One does not have to be a medical doctor or a public health professional to clearly think of measures, consequences, and adequacy of efforts in this arena.
Both the acts of commission and acts of omission in this domain will come to haunt us in the long run. History will tell if we were successful or not.
If the unfortunate nurse, the second to contract Ebola, had been given sufficient and correct knowledge of the potential risks for herself and others by her infectious disease specialists under whose supervision she had worked in that capacity, most likely she would not have engaged in such risky behavior. If she was indeed given such knowledge, her foolhardiness in undertaking air travel would be likely looked upon as an irresponsible act. It is clear that this brave woman was clearly misled by the CDC, therefore. Yet, no one can predict how many there are like her, who might unknowingly present danger of spreading Ebola virus by simply innocently not being aware of their being contagious. Of course, at the same time, we should leave room for some irresponsible or careless individuals who are in denial or simply throwing caution to the wind. With all that said, we are extremely grateful to the two nurses
who placed their life on line to treat the Ebola victims in Dallas and they will go down in the history
for their courage and sacrifice. Nothing said here should be interpreted as diminishing their
importance and in recognizing their stellar dedication to their profession.
However, if such is the case of an educated and trained nurse in a reputable high-tech hospital in Dallas, one should worry that CDC and infectious disease specialists have failed in educating
health care professionals even in the premier tertiary health care centers. Furthermore, blaming the late
Mr. Duncan, a layperson with no medical background, for all the problems the U.S. now faces, and as mainstream media have taken it upon themselves to do, is out of place and unjustified.
All of the above prompted the following list of steps the US (and other countries) can and should be taking to ensure the proper and most efficient containment of the rapidly spreading Ebola virus, before it reaches pandemic stages.
I. So, what can be done to better ensure the safety of the healthcare providers and others who may come into contact with, or be treating patients with, Ebola? How can the US provide better information and awareness to the general public, to arm them with the information they need, consistently and up-to-date, to allow them to better protect themselves?
Are we doing enough to enable the unfortunate health care workers that could come in
contact with Ebola, as well as the general public? Are the current public and electronic media channels such as PBS and other TV channels, YouTube, Facebook, e-mail list-serves, etc., being utilized
effectively to educate the health professionals, and even the public, proactively without causing
unnecessary panic, while still providing adequate information about the disease and all the proper measures people can take to not catch this disease or spread it if they were to come in contact with it? Such knowledge needs to be disseminated from one official credible site and must be vigilantly updated every day. Only in this manner can the population of the U.S. be alerted and educated widely.
Electronic media is obviously the best way to disseminate this knowledge, but the outlets must be brought online immediately and officially by the appropriate monitoring body, whether that is the CDC or some other agency charged with this most important mission. And, the clock is ticking.
II. How can the US better protect healthcare providers treating Ebola, especially with regards to protective gear being issued (e.g., hazmat suits) and safe working environments?
Protective Gear
1. The protective gear issued to healthcare workers treating the possibility or actual existence of Ebola should be standardized, uniformly manufactured at one facility or more accredited facilities, and distributed by one approved agency. This should not become a commercial vested interest enterprise to be exploited by profit mongers. This is not something the U.S. can afford to outsource to China or India.
2. Until a complete control over this virulent viral disease is attained, protective gear should not be left to the choice of the "hospital." Moreover, as is becoming more prevalent, any “CYA” operations or practices on the part of hospitals to blackmail potential contacts among their health care professionals to extract a legal promise from them to continue to work in high risk areas such as emergency rooms or ICU’s under the threat of lay off if they were to not sign on the dotted line saying they have been furnished (non-standardized) protective gears should be banned immediately.
3. For such bio-protective gears, the term “hazmat" is a misnomer, as this term refers to protection from hazardous chemicals and chemical gases, fumes and vapors. Viruses are distinctly different in that they grow and multiply once in contact with living host, which chemicals do not do. Therefore,
bio-contamination is different from chemical contamination.
Each country and each facility should compare their protective gear being utilized in prevention and must be required to use the most effective gears that have evidence based effectiveness in prevention. There should be efforts to clearly list all similarities and differences among such gears and make them uniformly secure. For, indeed, these gears will soon need mass production for use all over the world, and targeted research done now to design the most effective and safest gear will payoff one-hundred fold in the long-run.
4. In all facilities in the tertiary treatment areas, namely in the emergency treatment areas and intensive care units, the staff must be screened by Homeland Security or other responsible governmental agency such as the FBI to prevent any deliberate mistakes or mischief in violating the rules for prevention, and under penalty of law to prevent acts of terrorism. Such individuals motivated to spread the disease,
hence sacrificing their own lives, would be akin to suicide bombers. Conversely, the brave honest staff who are cleared to provide treatment, and who do so selflessly, need to be handsomely rewarded for their willingness to work in the Ebola-hazardous areas, rather than be threatened with lay off as a punishment if they refuse to work in those areas.
5. The wearing and removing of the bio-protective suits should be video recorded at the Ebola treatment facilities in W. Africa, Nigeria, etc. and if technically correct, their techniques need to be used as training videos to be publicized through official sites on the Internet, such as CDC site. These videos and other CDC approved videos should be continually played in the areas where health-care professionals prepare themselves for caring for the sick persons who may be Ebola victims. In this age of e-education they need to be publicized on the Internet also for the entire population to watch so they feel secure that all safety measures are undertaken on their behalf by the government and CDC.
6. The wearing and removing of the protective gear should be captured by multiple video cameras at the treatment facilities (like NIH or Emory) and reviewed immediately afterwards by experts (if necessary around the country) to catch any mistakes or possible contamination points and events.
If such video monitoring were to be available, it would have caught the two nurses in their act and would have quickly prevented an expensive nightmare. The CDC did not take advantage of this
readily available resource. Hopefully the attorneys did not advise the CDC to not use such monitoring.
It can be seen as the intrusion in the privacy of the health care professional but could be in place with
previously obtained informed consent.
Creating Safe Working Environments
Starting with the basics, in order to create safe working environments that will ensure that the virus will not spread while being Ebola victims are treated, here are a few policies that must be implemented.
1. The rules for prevention need to be at least openly exhibited for all intensive care staff including the doctors, nurses and other health care professionals, janitors and custodians who can come in contact with contaminated materials and who are trained to discard and dispose of Ebola containing bio-waste in a secure manner, and sterilize or fumigate the entire real estate or at least the facilities.
2. There need to be engineering consultants who can ensure secure air circulation, both pressurized air currents and exhausts in areas that house Ebola infected persons. Micro-droplets of water or body fluids can contaminate air in the treatment areas and the contention that Ebola is not an airborne disease is a dogma that is not yet evidence based nor rigorously and unequivocally proven with certainty.
All of these above mentioned techniques and more of them need to be publicized as the "standard of care" to be followed by all health care facilities that may get recruited to treat Ebola patients.
3. Disaster prevention nurses will need to be appointed like infection control nurses already are in every hospital. Not much is known about the psychological trauma from this biological disaster victimizing the Ebola patients and their contacts, as well as their bereaved relatives. They will need to be treated in the University departments of psychiatry by professionals trained to treat trauma victims and traumatic bereavement. Such specialized treatment resources need to be in place all over the country. Ebola is potentially a major disaster. Moreover, even the mental health workers who treat the potential Ebola patients will need to be trained in the handling of protective gears.
4. The threat of frivolous lawsuits must be removed. Facilities need to be rewarded for coming forward to face this challenge, rather than allowed to be punished with threats of liability suits by “ambulance chasing” attorneys who are, themselves, creating a major threat and impeding the implementation of preventive measures in the containment of this epidemic. These shysters need to be kept out of the game statutorily or by executive order of the President in the cause of National Emergency, lest they cause even greater setbacks to the containment process of this dangerous virus.
Having said that, the usual forensic, legal and medico-legal mentality will need drastic change while facing the dangers of Ebola. Society cannot afford to be distracted and disorganized by millions of lawsuits. Remember the "plague" of attorneys on every block of the country profiting from liability suits was not of an epidemic proportion with the power block of trial attorneys in the days of "Typhoid Mary,” nor during the devastating epidemics of influenza and plague in the remote past. This "plague" is likely to compound the plague (Ebola epidemic) when the attorneys start flapping their wings in the administration of health measures rather than take a back seat and be benevolent consultants to health care professionals. They should not be allowed to aggressively drive the public health departments and their policies merely from the viewpoint of liability. Liability and preventing law suits is their paramount interests rather than the true safety of the public at large.
5. Taking into account numbers 3 and 4, above, if the situation worsens, it could be entirely possible that martial law and emergency laws may have to be initiated in order to keep these liability- and liberty-interest protecting attorneys out of the game, so that quarantines can be prompt and effective without the hindrance of legal obstacles and impediments.
Indeed, the lack of intrusive and interfering attorneys, and the low cost of quarantines are behind the success of the Nigerian government and ridding its country of the threat of Ebola. Nigeria was superior to the United States in this area recently, and it may be that there is a lot to learn from Nigeria.
Therefore, the US must be careful to not approach the Nigerians with its typical air of arrogance or superiority, and communications must remain respectful and humble, in light of their exceptional success in spite of meager means compared to the U.S.’s CDC fumbling of the situation, thus far.
The US should learn exactly how the Nigerian government so effectively and quickly controlled and contained the threat of Ebola in that county, as well as how to scale their efforts to suit the US health care machine. Indeed, even if the U.S. comes up with a suitable bio-protective gear capable of being standardized, the gear should be compared to the ones used in W. Africa and Nigeria where effective containment of Ebola was demonstrated at least in the initial stages of this epidemic.
III. The Big Picture
While all of the above policy suggestions should be deemed imperative, a rapid response team and emergency measures are only half the answer; the team only reacts. What we need is also something more like a dedicated think tank - not a lethargic organization, but a dynamic pool of brainpower. The President did make efforts in this direction by appointing single competent administrator, i.e., Ebola Czar Ron Klain, to guide and direct all the public health measures, but more effort must be put forth, and on a grander scale.
Indeed, of all that is discussed in this article the key is awareness. The public's right to information would require that this new agency also become the information clearing-house to widely publish a daily official newsletter easily accessible to all to inform the citizens of the U.S. regarding daily updates. Taking full advantage of the e-media, TV channels, radio, etc. for general education of the public
and health care professionals needs to be given priority rather than making sweeping misleading
statements on air until all of us know all the tracks of the Ebola virus. Let us not be sufficiently content
with the rhetoric to prevent public panic and/or outrage, not at least until the disease is globally eradicated entirely like smallpox and polio.
Information should be readily available in the form of the following: (Preferably, on a readily accessible website like www.cdc.gov.org/ebola )
1) Currently identified Ebola patients who are receiving treatment and in what facilities
2) Number of Ebola exposed potential persons at risk and their geographic locations
and what is being offered to them to prevent their becoming symptomatic and/or
their becoming contagious presenting future risk to public in their incubation period.
3) All the individuals, their numbers and locations currently in isolation or quarantine
4) Updated treatment guidelines for the treatment of Ebola patients with guidelines
implemented for the protection of caregivers and potential contacts and their locations
5) Travel restrictions if any imposed on any of the ports of entry, daily updates of such measures
or their absence
6) Guidelines for public to prevent exposure to Ebola
7) Guidelines for those suspected to have been exposed to seek prompt services from
experts at all levels of care without health insurance related restrictions or obstacles
for receiving appropriate care.
IV. Final Point
Finally, any euphoria about the technical superiority of our medical profession or apparent short-term victory over the sneaky but powerful Ebola virus is only "ebullience" and not a balanced approach to the challenge ahead of us. This short article deliberately stays away from the consequences of lack
of Universal Health Care coverage and uninsured potential victims of Ebola showing up in health care facilities operating at conscious and unconscious level by denying or simply not providing adequate care for the uninsured. This makes it imperative that special funding for selected tertiary care centers needs to be considered.
---------0---0---0---------
Dr. Shree Vinekar, MD, is Professor Emeritus at the University of Oklahoma College of Medicine
Dr. A. V. Lakshminarayanan is the former Associate Professor, Dept of Radiology, Univ of Alabama at Birmingham; Adjunct faculty, Dept. of Biomedical Engineering, Univ of Alabama at Birmingham, Birmingham, Alabama.
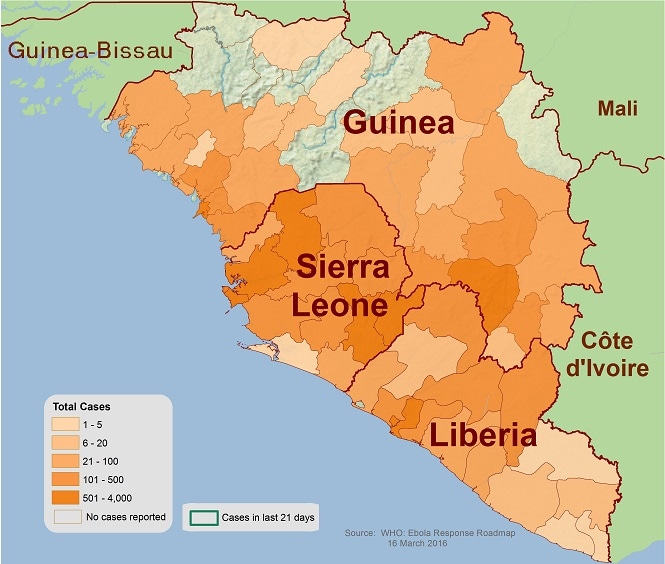
Case Counts
Case counts updated in conjunction with the World Health Organization updates and are based on information reported by the Ministries of Health.
As of November 18, 2014
(Updated November 24, 2014)
(Updated November 24, 2014)
Countries with Widespread Transmission
| Country | Total Cases | Laboratory-Confirmed Cases | Total Deaths |
|---|---|---|---|
| Guinea | 2047 | 1745 | 1214 |
| Liberia | 7082 | 2669 | 2963 |
| Sierra Leone | 6190 | 5152 | 1267 |
| Total | 15319 | 9566 | 5444 |
Countries with an Initial Case or Cases and/or Localized Transmission
| Country | Total Cases | Laboratory-Confirmed Cases | Total Deaths |
|---|---|---|---|
| United States | 4 | 4 | 1 |
| Mali | 6 | 5 | 6 |
| Total | 10 | 9 | 7 |
Previously Affected Countries
| Country | Total Cases | Laboratory-Confirmed Cases | Total Deaths |
|---|---|---|---|
| Nigeria* | 20 | 19 | 8 |
| Senegal* | 1 | 1 | 0 |
| Spain | 1 | 1 | 0 |
| Total | 22 | 21 | 8 |
Originally posted on Sunday October 19, 2014
Ebola e-Control vs. Ebola Ebullience: How to Implement Comprehensive Proactive Preventative Measures, Rather than Reactive Measures to Control the Ebola Epidemic and Avoid Law Suits from Potential Victims
By
Shree Vinekar, MD and A. V. Lakshminarayanan, PhD
First we should seriously acknowledge that Ebola infection is a terrible disease. We should not proclaim "we will stop Ebola in its tracks", which is a most vapid statement, to say the least. To say such things conveys an air of superiority over a mere virus and a sense of shortsightedness when dealing with a potential epidemic.
We do not have a full understanding of its lethal potential, virulent actions and preventive measures we should take, though the Center for Disease Control (CDC) is sincerely trying to gain some deeper understanding of these issues at the eleventh hour. However, as yet, we do not know its "tracks" – indeed, now the tracks are all over the US.
There are many assumptions being made about the spread of the disease. Some of the most important of these unknowns are:
·
One is that the affected person is not
contagious until symptomatic.
·
Second it is not an air-borne infection.
·
Third, body temperature alone is taken as the
determining criterion for who is symptomatic and who is not.
particularly from continent to continent, race to race, and also individual to individual, leave
alone the complexity of differential diagnoses of mild pyrexia. Triaging all patients with elevated
body temperature unnecessarily burdens the front line health care workers with a major dilemma.
This burden arises when thousands of people all over the country present with fever in
front line medical clinics and emergency rooms. Therefore, there need to be more specific criteria with
bio markers, if at all possible, to promptly implement detection and facilitate correct diagnosis of Ebola infection on all frontiers of health care, including public and private health care facilities.
Have we forgotten the history of "Typhoid Mary" in dealing with Ebola? Many "contacts" could be infectious a few days before they manifest recognizable symptoms of the Ebola infection not to mention that not all contacts will become alert enough to the dangers of the infection in a timely fashion to present themselves in a clinic or medical emergency room. There very well could be carriers of Ebola like, "typhoid Mary," who could go undetected as carriers until it is too late. Such dangers speak against complacence in our current ability to "stop Ebola in its tracks." The fact that 50% of the exposed individuals do not manifest illness of "Ebola infection" is in itself a red flag indicating the likelihood that many infectious persons may be running loose in society since having been already exposed to this virus.
One can very well understand the politically correct attitude of the government in not wanting to spread
panic while simultaneously providing primary and secondary prevention as well as excellent tertiary prevention and tertiary treatment centers all around the country. Even in this effort, however, the public is not entirely trusting of the governmental agencies responsible for this task.
Many individuals who were unfortunate to be on the same airplane as the Ebola patients likely feel they are not properly and promptly identified, nor given adequate information, nor sufficiently protected from the ensuing harm. Indeed, this feeling will linger at least for 21days, which is now strongly believed to be the incubation period for this infectious disease.
For example, the poor nurse who later tested positive for the Ebola infection, but who had been cleared for air travel by the CDC was sitting in the aisle in the airplane. Many other passengers could have rubbed against her if she was sitting in the aisle. Indeed, had she been sitting in a window or middle seat, it would have been nearly impossible to not come in contact with her fellow seatmates. Regardless, it was an act of commission with full knowledge that she was a participant in providing care for an Ebola victim.
And, yet, to isolate, quarantine, and monitor only those who sat close to the stricken nurse in the plane is very near-sighted. If she went to the toilet facilities, in the airplane or at the airports, very many more should be watched. Also what happened to the cups or utensils used by the person, either in the aircraft or at the airports? There are many more aspects to this specific public health expertise related skills that are simply dictated by common sense, that the people involved in guarding the public health in this country seem to be direly lacking in them or have not demonstrated that they possess these. One does not have to be a medical doctor or a public health professional to clearly think of measures, consequences, and adequacy of efforts in this arena.
Both the acts of commission and acts of omission in this domain will come to haunt us in the long run. History will tell if we were successful or not.
If the unfortunate nurse, the second to contract Ebola, had been given sufficient and correct knowledge of the potential risks for herself and others by her infectious disease specialists under whose supervision she had worked in that capacity, most likely she would not have engaged in such risky behavior. If she was indeed given such knowledge, her foolhardiness in undertaking air travel would be likely looked upon as an irresponsible act. It is clear that this brave woman was clearly misled by the CDC, therefore. Yet, no one can predict how many there are like her, who might unknowingly present danger of spreading Ebola virus by simply innocently not being aware of their being contagious. Of course, at the same time, we should leave room for some irresponsible or careless individuals who are in denial or simply throwing caution to the wind. With all that said, we are extremely grateful to the two nurses
who placed their life on line to treat the Ebola victims in Dallas and they will go down in the history
for their courage and sacrifice. Nothing said here should be interpreted as diminishing their
importance and in recognizing their stellar dedication to their profession.
However, if such is the case of an educated and trained nurse in a reputable high-tech hospital in Dallas, one should worry that CDC and infectious disease specialists have failed in educating
health care professionals even in the premier tertiary health care centers. Furthermore, blaming the late
Mr. Duncan, a layperson with no medical background, for all the problems the U.S. now faces, and as mainstream media have taken it upon themselves to do, is out of place and unjustified.
All of the above prompted the following list of steps the US (and other countries) can and should be taking to ensure the proper and most efficient containment of the rapidly spreading Ebola virus, before it reaches pandemic stages.
I. So, what can be done to better ensure the safety of the healthcare providers and others who may come into contact with, or be treating patients with, Ebola? How can the US provide better information and awareness to the general public, to arm them with the information they need, consistently and up-to-date, to allow them to better protect themselves?
Are we doing enough to enable the unfortunate health care workers that could come in
contact with Ebola, as well as the general public? Are the current public and electronic media channels such as PBS and other TV channels, YouTube, Facebook, e-mail list-serves, etc., being utilized
effectively to educate the health professionals, and even the public, proactively without causing
unnecessary panic, while still providing adequate information about the disease and all the proper measures people can take to not catch this disease or spread it if they were to come in contact with it? Such knowledge needs to be disseminated from one official credible site and must be vigilantly updated every day. Only in this manner can the population of the U.S. be alerted and educated widely.
Electronic media is obviously the best way to disseminate this knowledge, but the outlets must be brought online immediately and officially by the appropriate monitoring body, whether that is the CDC or some other agency charged with this most important mission. And, the clock is ticking.
II. How can the US better protect healthcare providers treating Ebola, especially with regards to protective gear being issued (e.g., hazmat suits) and safe working environments?
Protective Gear
1. The protective gear issued to healthcare workers treating the possibility or actual existence of Ebola should be standardized, uniformly manufactured at one facility or more accredited facilities, and distributed by one approved agency. This should not become a commercial vested interest enterprise to be exploited by profit mongers. This is not something the U.S. can afford to outsource to China or India.
2. Until a complete control over this virulent viral disease is attained, protective gear should not be left to the choice of the "hospital." Moreover, as is becoming more prevalent, any “CYA” operations or practices on the part of hospitals to blackmail potential contacts among their health care professionals to extract a legal promise from them to continue to work in high risk areas such as emergency rooms or ICU’s under the threat of lay off if they were to not sign on the dotted line saying they have been furnished (non-standardized) protective gears should be banned immediately.
3. For such bio-protective gears, the term “hazmat" is a misnomer, as this term refers to protection from hazardous chemicals and chemical gases, fumes and vapors. Viruses are distinctly different in that they grow and multiply once in contact with living host, which chemicals do not do. Therefore,
bio-contamination is different from chemical contamination.
Each country and each facility should compare their protective gear being utilized in prevention and must be required to use the most effective gears that have evidence based effectiveness in prevention. There should be efforts to clearly list all similarities and differences among such gears and make them uniformly secure. For, indeed, these gears will soon need mass production for use all over the world, and targeted research done now to design the most effective and safest gear will payoff one-hundred fold in the long-run.
4. In all facilities in the tertiary treatment areas, namely in the emergency treatment areas and intensive care units, the staff must be screened by Homeland Security or other responsible governmental agency such as the FBI to prevent any deliberate mistakes or mischief in violating the rules for prevention, and under penalty of law to prevent acts of terrorism. Such individuals motivated to spread the disease,
hence sacrificing their own lives, would be akin to suicide bombers. Conversely, the brave honest staff who are cleared to provide treatment, and who do so selflessly, need to be handsomely rewarded for their willingness to work in the Ebola-hazardous areas, rather than be threatened with lay off as a punishment if they refuse to work in those areas.
5. The wearing and removing of the bio-protective suits should be video recorded at the Ebola treatment facilities in W. Africa, Nigeria, etc. and if technically correct, their techniques need to be used as training videos to be publicized through official sites on the Internet, such as CDC site. These videos and other CDC approved videos should be continually played in the areas where health-care professionals prepare themselves for caring for the sick persons who may be Ebola victims. In this age of e-education they need to be publicized on the Internet also for the entire population to watch so they feel secure that all safety measures are undertaken on their behalf by the government and CDC.
6. The wearing and removing of the protective gear should be captured by multiple video cameras at the treatment facilities (like NIH or Emory) and reviewed immediately afterwards by experts (if necessary around the country) to catch any mistakes or possible contamination points and events.
If such video monitoring were to be available, it would have caught the two nurses in their act and would have quickly prevented an expensive nightmare. The CDC did not take advantage of this
readily available resource. Hopefully the attorneys did not advise the CDC to not use such monitoring.
It can be seen as the intrusion in the privacy of the health care professional but could be in place with
previously obtained informed consent.
Creating Safe Working Environments
Starting with the basics, in order to create safe working environments that will ensure that the virus will not spread while being Ebola victims are treated, here are a few policies that must be implemented.
1. The rules for prevention need to be at least openly exhibited for all intensive care staff including the doctors, nurses and other health care professionals, janitors and custodians who can come in contact with contaminated materials and who are trained to discard and dispose of Ebola containing bio-waste in a secure manner, and sterilize or fumigate the entire real estate or at least the facilities.
2. There need to be engineering consultants who can ensure secure air circulation, both pressurized air currents and exhausts in areas that house Ebola infected persons. Micro-droplets of water or body fluids can contaminate air in the treatment areas and the contention that Ebola is not an airborne disease is a dogma that is not yet evidence based nor rigorously and unequivocally proven with certainty.
All of these above mentioned techniques and more of them need to be publicized as the "standard of care" to be followed by all health care facilities that may get recruited to treat Ebola patients.
3. Disaster prevention nurses will need to be appointed like infection control nurses already are in every hospital. Not much is known about the psychological trauma from this biological disaster victimizing the Ebola patients and their contacts, as well as their bereaved relatives. They will need to be treated in the University departments of psychiatry by professionals trained to treat trauma victims and traumatic bereavement. Such specialized treatment resources need to be in place all over the country. Ebola is potentially a major disaster. Moreover, even the mental health workers who treat the potential Ebola patients will need to be trained in the handling of protective gears.
4. The threat of frivolous lawsuits must be removed. Facilities need to be rewarded for coming forward to face this challenge, rather than allowed to be punished with threats of liability suits by “ambulance chasing” attorneys who are, themselves, creating a major threat and impeding the implementation of preventive measures in the containment of this epidemic. These shysters need to be kept out of the game statutorily or by executive order of the President in the cause of National Emergency, lest they cause even greater setbacks to the containment process of this dangerous virus.
Having said that, the usual forensic, legal and medico-legal mentality will need drastic change while facing the dangers of Ebola. Society cannot afford to be distracted and disorganized by millions of lawsuits. Remember the "plague" of attorneys on every block of the country profiting from liability suits was not of an epidemic proportion with the power block of trial attorneys in the days of "Typhoid Mary,” nor during the devastating epidemics of influenza and plague in the remote past. This "plague" is likely to compound the plague (Ebola epidemic) when the attorneys start flapping their wings in the administration of health measures rather than take a back seat and be benevolent consultants to health care professionals. They should not be allowed to aggressively drive the public health departments and their policies merely from the viewpoint of liability. Liability and preventing law suits is their paramount interests rather than the true safety of the public at large.
5. Taking into account numbers 3 and 4, above, if the situation worsens, it could be entirely possible that martial law and emergency laws may have to be initiated in order to keep these liability- and liberty-interest protecting attorneys out of the game, so that quarantines can be prompt and effective without the hindrance of legal obstacles and impediments.
Indeed, the lack of intrusive and interfering attorneys, and the low cost of quarantines are behind the success of the Nigerian government and ridding its country of the threat of Ebola. Nigeria was superior to the United States in this area recently, and it may be that there is a lot to learn from Nigeria.
Therefore, the US must be careful to not approach the Nigerians with its typical air of arrogance or superiority, and communications must remain respectful and humble, in light of their exceptional success in spite of meager means compared to the U.S.’s CDC fumbling of the situation, thus far.
The US should learn exactly how the Nigerian government so effectively and quickly controlled and contained the threat of Ebola in that county, as well as how to scale their efforts to suit the US health care machine. Indeed, even if the U.S. comes up with a suitable bio-protective gear capable of being standardized, the gear should be compared to the ones used in W. Africa and Nigeria where effective containment of Ebola was demonstrated at least in the initial stages of this epidemic.
III. The Big Picture
While all of the above policy suggestions should be deemed imperative, a rapid response team and emergency measures are only half the answer; the team only reacts. What we need is also something more like a dedicated think tank - not a lethargic organization, but a dynamic pool of brainpower. The President did make efforts in this direction by appointing single competent administrator, i.e., Ebola Czar Ron Klain, to guide and direct all the public health measures, but more effort must be put forth, and on a grander scale.
Indeed, of all that is discussed in this article the key is awareness. The public's right to information would require that this new agency also become the information clearing-house to widely publish a daily official newsletter easily accessible to all to inform the citizens of the U.S. regarding daily updates. Taking full advantage of the e-media, TV channels, radio, etc. for general education of the public
and health care professionals needs to be given priority rather than making sweeping misleading
statements on air until all of us know all the tracks of the Ebola virus. Let us not be sufficiently content
with the rhetoric to prevent public panic and/or outrage, not at least until the disease is globally eradicated entirely like smallpox and polio.
Information should be readily available in the form of the following: (Preferably, on a readily accessible website like www.cdc.gov.org/ebola )
1) Currently identified Ebola patients who are receiving treatment and in what facilities
2) Number of Ebola exposed potential persons at risk and their geographic locations
and what is being offered to them to prevent their becoming symptomatic and/or
their becoming contagious presenting future risk to public in their incubation period.
3) All the individuals, their numbers and locations currently in isolation or quarantine
4) Updated treatment guidelines for the treatment of Ebola patients with guidelines
implemented for the protection of caregivers and potential contacts and their locations
5) Travel restrictions if any imposed on any of the ports of entry, daily updates of such measures
or their absence
6) Guidelines for public to prevent exposure to Ebola
7) Guidelines for those suspected to have been exposed to seek prompt services from
experts at all levels of care without health insurance related restrictions or obstacles
for receiving appropriate care.
IV. Final Point
Finally, any euphoria about the technical superiority of our medical profession or apparent short-term victory over the sneaky but powerful Ebola virus is only "ebullience" and not a balanced approach to the challenge ahead of us. This short article deliberately stays away from the consequences of lack
of Universal Health Care coverage and uninsured potential victims of Ebola showing up in health care facilities operating at conscious and unconscious level by denying or simply not providing adequate care for the uninsured. This makes it imperative that special funding for selected tertiary care centers needs to be considered.
---------0---0---0---------
Dr. Shree Vinekar, MD, is Professor Emeritus at the University of Oklahoma College of Medicine
Dr. A. V. Lakshminarayanan is the former Associate Professor, Dept of Radiology, Univ of Alabama at Birmingham; Adjunct faculty, Dept. of Biomedical Engineering, Univ of Alabama at Birmingham, Birmingham, Alabama.
Enhanced Ebola Screening to Start at Five U.S. Airports and New Tracking Program for all People Entering U.S. from Ebola-affected Countries
New layers of screening at airports that receive more than 94% of West African Travelers

The Centers for Disease Control and Prevention (CDC) and the Department of Homeland Security's Customs & Border Protection (CBP) this week will begin new layers of entry screening at five U.S. airports that receive over 94 percent of travelers from the Ebola-affected nations of Guinea, Liberia, and Sierra Leone.
New York's JFK International Airport will begin the new screening on Saturday. In the 12 months ending July 2014, JFK received nearly half of travelers from the three West African nations. The enhanced entry screening at Washington-Dulles, Newark, Chicago-O'Hare, and Atlanta international airports will be implemented next week.
"We work to continuously increase the safety of Americans," said CDC Director Tom Frieden, M.D., M.P.H. "We believe these new measures will further protect the health of Americans, understanding that nothing we can do will get us to absolute zero risk until we end the Ebola epidemic in West Africa."
"CBP personnel will continue to observe all travelers entering the United States for general overt signs of illnesses at all U.S. ports of entry and these expanded screening measures will provide an additional layer of protection to help ensure the risk of Ebola in the United States is minimized," said Secretary of Homeland Security Jeh Johnson. "CBP, working closely with CDC, will continue to assess the risk of the spread of Ebola into the United States, and take additional measures, as necessary, to protect the American people."
CDC is sending additional staff to each of the five airports. After passport review:
- Travelers from Guinea, Liberia, and Sierra Leone will be escorted by CBP to an area of the airport set aside for screening.
- Trained CBP staff will observe them for signs of illness, ask them a series of health and exposure questions and provide health information for Ebola and reminders to monitor themselves for symptoms. Trained medical staff will take their temperature with a non-contact thermometer.
- If the travelers have fever, symptoms or the health questionnaire reveals possible Ebola exposure, they will be evaluated by a CDC quarantine station public health officer. The public health officer will again take a temperature reading and make a public health assessment. Travelers, who after this assessment, are determined to require further evaluation or monitoring will be referred to the appropriate public health authority.
- Travelers from these countries who have neither symptoms/fever nor a known history of exposure will receive health information for self-monitoring.
Entry screening is part of a layered process that includes exit screening and standard public health practices such as patient isolation and contact tracing in countries with Ebola outbreaks. Successful containment of the recent Ebola outbreak in Nigeria demonstrates the effectiveness of this approach.
These measures complement the exit screening protocols that have already been implemented in the affected West African countries, and CDC experts have worked closely with local authorities to implement these measures. Since the beginning of August, CDC has been working with airlines, airports, ministries of health, and other partners to provide technical assistance for the development of exit screening and travel restrictions in countries affected by Ebola. This includes:
- Assessing the capacity to conduct exit screening at international airports;
- Assisting countries with procuring supplies needed to conduct exit screening;
- Supporting with development of exit screening protocols;
- Developing tools such as posters, screening forms, and job-aids; and
- Training staff on exit screening protocols and appropriate personal protective equipment (PPE)
Today, all outbound passengers are screened for Ebola symptoms in the affected countries. Such primary exit screening involves travelers responding to a travel health questionnaire, being visually assessed for potential illness, and having their body temperature measured. In the last two months since exit screening began in the three countries, of 36,000 people screened, 77 people were denied boarding a flight because of the health screening process. None of the 77 passengers were diagnosed with Ebola and many were diagnosed as ill with malaria, a disease common in West Africa, transmitted by mosquitoes and not contagious from one person to another.
Exit screening at airports in countries affected by Ebola remains the principal means of keeping travelers from spreading Ebola to other nations. All three of these nations have asked for, and continue to receive, CDC assistance in strengthening exit screening.
Hemant Sashittal: You are very charitable; and your words are very kind; mankind has little hope if it depends on my skills or intelligence. The CDC needs to speak with authority and in a confident voice; they have not. We did no service by questioning the CDC chief in a way to make him look like a chump. I am sure he is a smart man, and he was learning quickly. Humiliating him publicly was a political stunt that will cost us. The challenge (in the least) is of disseminating clear information and training to front line workers, ensuring people have authority to quarantine people when necessary, and an impossible task of managing the logistics of containment, delivery of medicines, and administering of care in isolation units. Marketers obsess over logistics; we can help in this regard (mostly converts from math and engineering who went on to study logistics). Social media, GPS on cell phones, Twitter traffic, Facebook posts - can all help identify hotspots with a potential for spreading disease. The popular press has helped spread hysteria; we need the pharma industry to spread information (they spend more money on marketing than on developing and testing drugs). They have an infrastructure of sales persons in place; they can carry the message to every single health care facility faster than anyone. People are discussing possibilities (it is possible) and not probabilities. If we were focused on the latter (as your notes suggest), despite the tragedies, we can actively reduce probability of an epidemic. But, that would require us to operate from the realm of knowledge and not belief, from science and not superstition, and from the voices of doctors and epidemiologists and not fear mongers.
ReplyDeleteHemant Sashittal, PhD
Professor of Marketing
Sanju Vinekar wrote:
ReplyDeleteU.S. Ebola Case #4:
So, this young helpful American doctor returns home after treating Ebola patients in Guinea ... and he could have laid low for 21 days, like folks are supposed to do after exposure.
But, instead, he had a much more fun idea. He decided to go out on the town, ride the NYC subway, and then go bowling. Then he came down with Ebola symptoms the very next day.
Save a few in Guinea and then come home and infect NYC. Smart.
#MCATmissingcommonsensesection